
Getting your posture right
In the current climate, one where we many of us were forced to be out of work for 3 months (alongside so many globally), I have never been more concerened with ensuring I am fit and healthy to work until the day I plan to retire. The sudden inability to be able to earn a living was a huge wake up call and I will never take the absolute privilege to work for granted again. Whilst putting into place plans to be able to survive another pandemic or similar that could deem me out of work I will be ensuring my personal health, fitness, as well as physical ability and overall wellness is a priority.
In light of this concept, thinking back to my time training to be a dental hygienist I can remember how often we were warned about posture and how to preserve our back. As I was in my early twenties I didn’t consider it a problem at the time. I did what was asked of me in the dental schools’ clinical environment of course, I was being watched by a handful of clinic tutors at all times, so I abided by every rule. Getting out into general practice however was a different story. With time constraints and clinical pressures, I found myself using direct vision more and the only time I really ever considered my back and neck health again is when it started to ache. I then adopted a better posture until I didn’t have pain and the same cycle continued. Does this sound familiar?
As I am now over 10 years qualified, I find that I am having to make this call far more often and it has made me question myself… should I be adopting good back and neck posture at all times if I don’t want to end up having spinal disc issues or worse later in my life? The answer of course is yes. I am actually sick of the pain, which now leads to frequent headaches on a weekly basis. It isn’t until you really start to delve deeper into this concept that you find it may all be interrelated and stems from poor posture.
A study carried out about back and neck pain within dentistry in 2018 by Ajwa. N et al found that 70% of the surveyed dental professionals reported back pain, with lower back pain being the most reported problem, contributing to 46.7% of the claims. Interestingly this did not correlate to the number of patients seen in a day, it was a common issue regardless of patient numbers. Another study by Chadra et al found that 73% suffered back pain and 40% suffered neck pain. This is a common issue within dentistry. In both studies the head, neck and back complaints were put down to poor posture during working hours. What was also surprising is that even though the majority of the surveyed professionals suffered neck and back pain, they actually admitted to knowing the advantages of assistive stools but less than 50% used them.
The issue with poor posture is that over time it can lead to placing an overload onto the lower spinal discs, causing them to herniate. In dentistry it is well documented that frequent tension headaches and head and neck pain are common, of which can be a result of prolonged elevation of the shoulders resulting in trapezius myalgia. Do you ever suffer from a headache above one of the eyes whilst also in the correlating temple region simultaneously? It could be the upper trapezius that is the culprit. Mental stress, infrequent breaks, poor posture and poor head position is to blame.
If you’re like me and you have decided that you want to do all you can to prevent further or future problems there is some good news. There are a few things you can start doing to help preserve your back and prevent the pain.
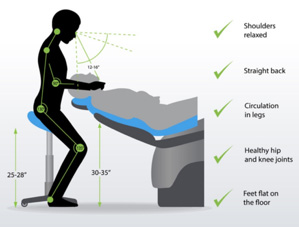
- Walk tall- Walk like a puppeteer has some string attached to the top of your head and they are pulling you up. Have your head balanced above your spine and shoulders pulled back and relaxed.
- Choose back support- When you are sitting to work and you prefer a chair, choose one with a back support and sit with your back flush with the back rest. Preferably choose a chair which is slightly tilted forwards. A forward leaning seat helps to maintain the natural curvature of the spine and is the most suitable for longer periods of sitting. A great option is the Belmont ic-Tilt. You should also bend your arms 75- 90 degrees at the elbow and keep your legs hip distance apart with your feet planted flat on the floor if not needing to use the foot peddle.
- Choose a saddle stool- The whole idea behind a saddle stool is to create a good posture, strengthen the core and reduce back pain. It is shaped like an equestrian saddle after it was found that this unique shape put the user in a forward leaning position bending the knees and hips at about 135 degrees. This is optimum for taking pressure off the lower spine and preventing lower back pain. A systemic review was carried out by Gouvea. G and results showed that ‘saddle seats were associated with a significantly lower ergonomic risk than conventional seats indicating postural improvement’. A great option is the Belmont saddle stool with a tilting seat to allow for a forward leaning position as recommended.
- Posture improving stretches- You can perform stretches during the day while sat in your chair at work to counteract the posture you find yourself in for most of the day. (See photos).
- Strengthen your core- Your core supports your spine, so strong abdominal and deep core muscles take the pressure off your back and help align your spine. This can ease any back pain and prevent further injury or strain.
When considering your posture during treatment there are 3 main things you need to consider:
- Operator position
- Chair height
- Patient position

Let us first look at chair height and the different locations in the mouth you are wanting to access. Something that is often disregarded while we are in the zone during treatment is the fact we should be adjusting our working position and/or patient position to focus on different areas of the mouth.
- For maxillary teeth, the chair height should be 8cm below the shoulder level of the operator.
- For mandibular teeth, the chair height should be 16cm below the level of the operators elbow.
Next we should consider the operator position based on the maxillary and mandibular arches. This differs if you are left or right- handed and is discussed below as if looking at a clock face:
- Right-handed clinicians should work around the 9, 10, 11, 12 o’clock positions (when thinking of a clock face).
- Left-handed clinicians should work around the 12, 1, 2, 3 o’clock positions (when thinking of a clock face).


And finally, we look at the patients’ position. The patient will almost always be in a supine position unless there is a medical reason that would deem the patient unable to reach this most satisfactory operating position for the clinician. Wherever possible though, the clinician should try to have the patient laid supinely to save pressure on their own back.
- For maxillary teeth the back of the chair should be slightly 45 degrees from the floor and the patient should be placed in a chin up position
- For mandibular teeth the back of the chair should be almost parallel to the floor and the patient should be placed in a chin down position
Because in dentistry we see numerous patients on a daily basis, or carry out lengthy treatments on individual cases, it is very easy to become complacent with our own back and neck/shoulder care and we cease to adjust our working position throughout treatment in order to make the appointment more efficient, time wise. That is why it is extremely important to consider not just the chair that you are sat on during treatment, but the chair in which the patient is to be sat. For example, the Belmont Clesta II chair features 2 preset positions (perfect if up to 2 clinicians utilise the same surgery space) and a last position memory function on an 8- way foot control. This eases the ability to adjust according to your own dimensions throughout treatment and allows the ability for numerous clinicians to use the same chair without compromising their back health.
By choosing a Belmont surgery system such as the tb Compass ‘Surgery System’, you have access to an ambidextrous unit that can be adjusted for right and left-handed clinicians and 4 programmable operator settings. Or the Clesta II Holder Type system with assistants console to further help the clinician achieve adequate height adjustment throughout treatment as necessary. The detachable cuspidor bowl with a 90-degree outward rotation is also a handy feature, despite often being over-looked. This chair also has a right or left-handed installation option for more permanent operator positions (perfect for when a more fixed position is required and the same clinician is solely utilising the surgery space).
One thing I consider when I am buying a new mattress is I spend a vast majority of my life in bed and so it is important to invest in one that supports me in the best possible way. The same concept applies to investing in something we spend a vast amount of time doing, working in clinical practice in a seated position for long periods, often in stressful positions. And although patient comfort and aesthetics are extremely important, do not over-look what a well-considered chair, chair system and stool can offer you and your team, for yours and their comfort and take the time to ensure you manage and consider your back and neck health.
References:
Ajwa N et al. ‘Neck and back pain as reported by dental practitioners in Riyadh city’. Published August 30, 2018. Journal of Dental Health Oral Disorders and Therapy
Gouvea G. Assessment of the ergonomic risk from saddle and conventional seats in dentistry: A systematic review and meta analysis’. Published online 17 Dec, 2018. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6296655/